
Everything You Need to Know About America’s National COVID-19 Preparedness Plan (Part 2)
Part 2

America’s updated COVID-19 preparedness plan was just released by the White House on March 2nd, 2022. I decided to undertake the task of briefing this document to summarize its main points. This way I carry the burden of subjecting myself to Biden’s insanity, while also providing you with the latest on America’s COVID-19 preparedness. You can reference the National COVID-19 Preparedness Plan here: https://www.whitehouse.gov/wp-content/uploads/2022/03/NAT-COVID-19-PREPAREDNESS-PLAN.pdf. Underneath each quoted sample of the document, you will find my analysis and interpretation on statements that came directly from the White House.
Pg.29) “…NIH is also developing new vaccine platforms and multivalent immunogens; and NIH – in close collaboration with Biomedical Advanced Research and Development Authority (BARDA) – is supporting research and facilitating advanced development of promising candidates.”
Pg.66) “Strengthen partnerships to prepare for the effective global surveillance of variants…These efforts will be coordinated through the SARS-COV-2 Interagency Group (SIG) which includes experts from BARDA, CDC, DOD, FDA, HHS, NIH and the Department of Agriculture (USDA), who collaborate to continuously monitor and assess emerging variants in the United States and around the world.”
Pg.68) “Strengthen existing collaborations with providers of genetic sequence and analysis and our network of labs so the government can immediately test the effectiveness of our vaccines, treatments, and tests. The federal government – coordinating with CDC, NIH, BARDA, and FDA…”
It comes as no surprise that BARDA continues to emerge as a driving force behind America’s COVID preparedness plan. The current director of BARDA is Dr. Gary Disbrow. There are many suspicious players involved in this operation, one of which is Dawn O’Connell who currently serves as the Assistant Secretary for Preparedness and Response (ASPR) for HHS (Department of Health and Human Services). The following discussion between Dr. Disbrow and Dawn O’Connell outline some of the very same topics covered within the National Covid Preparedness Plan…
If we do a little bit of digging on Dawn O’Connell, we come to find a connection between her and the infamous Peter Daszak. In case your memory needs refreshing, Peter Daszak not only covered up the fact that the COVID-19 virus originated in the Wuhan lab, but also generously sent your tax dollars to laboratories who support “gain of function” research. As O’Connell was working with the Coalition for Epidemic Preparedness Innovations (CEPI), back in December of 2019 (coincidentally the same time period the world recorded its first COVID-19 outbreak from Wuhan China), she attended the Nipah Virus International Conference in Singapore. The conference was funded in part by the Bill and Malinda Gates foundation and organized by CEPI, the World Health Organization (WHO), The National Institute of Allergy and Infectious Diseases (NIAID), and Duke-Nus Medical School. Notable attendees, alongside O’Connell, included Peter Daszak (President of EcoHealth Alliance), the Wuhan “bat lady” Shi Zhengli, and Hume Field (Advisor for EcoHealth Alliance). (https://web.archive.org/web/20210329222025/https://nipah2019.miceapps.com/client/sites/page/503/1389) Not much has changed since this time, as we see the Biden Administration continue to support organizations like BARDA/ASPIR and individuals like Dawn O’Connell who coincidentally attend conferences with Peter Daszak. One interesting side note, about the Nipah conference, is that Peter Daszak deleted the following tweet sent out on the last day of the conference…
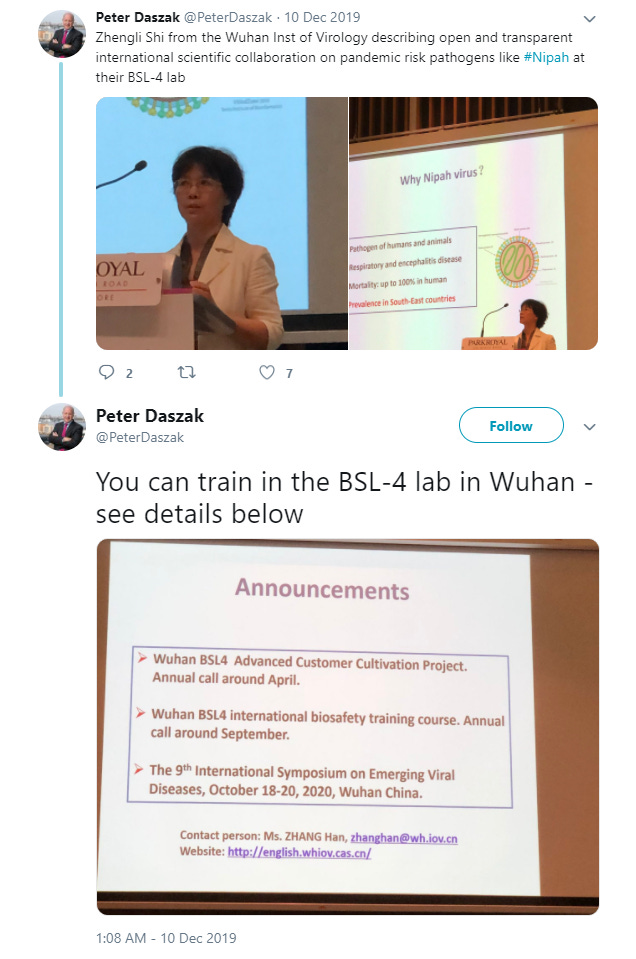
It seems as though this post incriminates Daszak as it draws a connection (pre-COVID outbreak) between him and the Wuhan Institute of Virology. The Nipah conference logo is another noteworthy coincidence worth pointing out. Within the “20” font below, you find a depiction of spike protein and what appears to be a Wuhan market disease ridden bat. It seems as if the individuals who organized this conference had already developed a pre-conceived origin story for the COVID-19 outbreak?

***
Pg.44) “Continue innovation through investments in existing technologies. The Administration has accelerated the NIH Rapid Acceleration of Diagnostics RADx technology program that continues to work with government scientists, academic research organizations, and the private sector.”
The National Institutes of Health (NIH) Rapid Acceleration of Diagnostics Tech (RADx Tech) program, “…aims to speed the development, validation, and commercialization of innovative point-of-care and home-based tests, as well as improve clinical laboratory tests, that can directly detect the virus.” (https://www.nih.gov/research-training/medical-research-initiatives/radx/radx-programs) The RADx programs have already failed miserably with COVID testing. Not to worry though! The Biden administration plans to reward RADx with more tax dollars. Who throws money down at technologies that fail? Well, I suppose it depends on whether you think RADx programs are successful or not? Maybe the Biden Administration simply rewards RADx for successfully contributing to the staged, fraudulent, artificial “plandemic” which won Biden the 2020 presidential election? It is already known that the initial COVID-19 PCR tests were wildly inaccurate, via false positive results, and did not represent an honest case count back in 2020 and 2021. The NIH, back in October of 2020, admitted that most BARDA testing options were not able to distinguish between influenza and SARS-COV-2. “BARDA has contributed substantially to the nation’s COVID testing capacity with development support of 30 SARS-COV-2 diagnostic tests since March (2020), 15 of which have achieved FDA emergency use authorization (EUA). Five of the 30 tests can distinguish between influenza and SARS-COV-2, the virus that causes COVID-19, from the same sample, and two of those have achieved EUA.” (https://www.nih.gov/news-events/news-releases/nih-radx-initiative-advances-six-new-covid-19-testing-technologies) Notice how only 2 of the 15 EUA tests distinguish between COVID-19 and influenza. One would assume the NIH would ONLY promote these two testing options however, this was not the case. Today, RADx continues its focus on, “… (1) an antigen test that provides results in 15 mins, (2) a viral RNA test deployed in mobile vans that can travel to COVID hotspots…” (https://www.nih.gov/news-events/news-releases/nih-radx-initiative-advances-six-new-covid-19-testing-technologies) The most intriguing RADx program is called RADx Radical (RADx-rad). RADx-rad specializes in non-traditional approaches to COVID-19 testing. Some of these strategies include community wastewater analysis, surveillance methods for high-risk populations, home-based tests that detect sensory functions to predict disease, and “…artificial intelligence (AI) systems with novel biosensing or laboratory diagnostics with digital health technologies for screening, diagnosing, and monitoring COVID-19, including in children, and to predict disease severity”. (https://www.nih.gov/research-training/medical-research-initiatives/radx/radx-programs) In my mind, two key phrases instantly jump off the screen. “…surveillance methods for high-risk populations”, and “AI systems with novel biosensing diagnostics”. Is RADx-rad taking steps towards a “Black Mirror” (Netflix series) dystopian society?
Surely, RADx implementing AI, covid sensing, Black Mirror robot dogs is a stretch but, in reality, the concept is exactly the same. Any government funded program involving AI and surveillance should frighten each and every one of us. Undoubtedly, the money dished out to RADx programs, to the tune of 1.5 billion (https://www.nih.gov/research-training/medical-research-initiatives/radx/radx-programs) for COVID-19 testing and surveillance, raises suspicions considering their past inadequacies during the COVID-19 era.
***
Pg.47) The Administration will continue to center communities of color and other underserved populations in the design of all COVID-19 initiatives; address COVID-related health inequities among communities defined by race, ethnicity, geography, disability, sexual orientation, gender identity, and other factors; and partner with Tribal nations, Indigenous communities and rural communities to design equitable initiatives.
Pg.56) Support community-based organizations to expand vaccination and boosters to underserved groups.
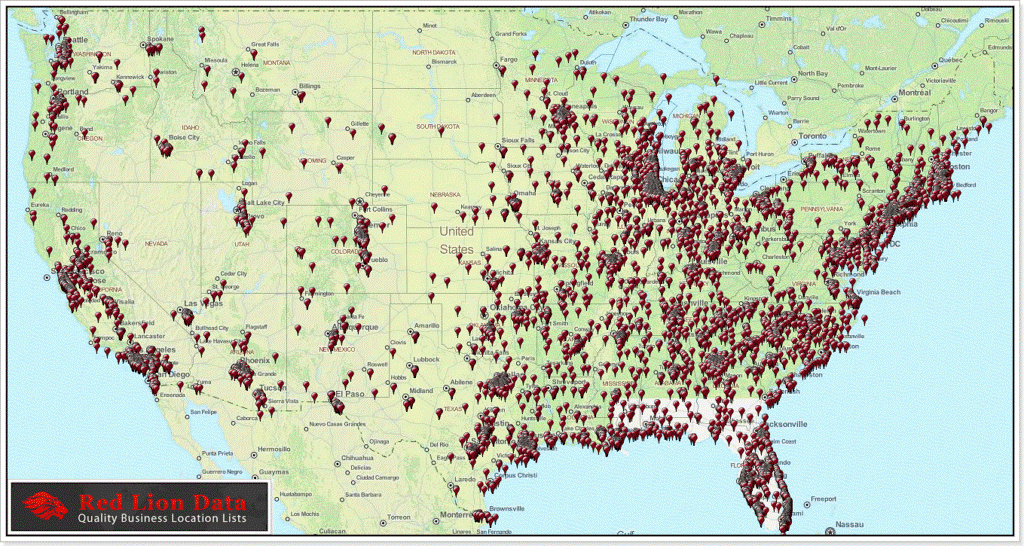
These equity/underserved population sections, within the preparedness plan, confuse me, agitate me, and motivate me. I am not sold on the fact that “underserved” populations have limited access to COVID-19 testing or vaccines. The following maps depict Walgreens and CVS store locations, throughout the United States, that serve our community…
Walgreens Store Location Map
CVS Store Location Map
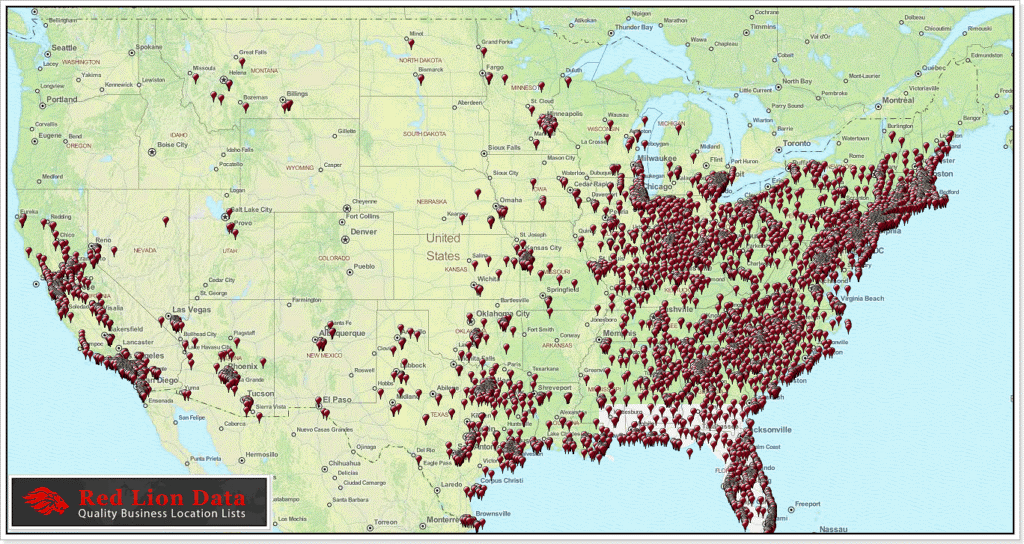
If we look at locations for one pharmacy chain and combine it with the number of hospitals/health care facilities nationwide, clearly, the availability for COVID treatment exists.
The Native American population is a recurring point of focus within the COVID preparedness plan. It turns out that indigenous communities are vaccine hesitant and their resistance against big pharma is not acceptable in the eyes of Uncle Sam. I think we all know why Native American distrust our government in the first place and they have good reason…
Mainstream media (MSM) force feeding a toxic narrative does not help matters. Health Affairs published a perfect example of cringe worthy MSM hogwash as America exploits a segment of our society once again… https://www.healthaffairs.org/do/10.1377/forefront.20210723.390196/. The lack of reverence and condescending attitude towards the Native American culture, knowledge, and tradition is on full display within this article. We start to grasp another sinister motive behind America’s newest “medical tyranny” preparedness plan. Here is a real-life Native American perspective, within the comments section, underneath Health Affair’s abhorrent article…
“Why are you people working so dang hard to inoculate a population of people that don’t want it (COVID vaccine)? Seriously. Do you still think you know what’s best for us? That we need white people to get by?
My tribe’s vaccination rate is less than 30% because the US government has always come under benevolent auspices to screw us over, so most of us wish you all would just leave us alone already.
This will never get published because it doesn’t fit your narrative. We’ve been silenced before, too.”
*User—mthashp
Let’s stop with the disingenuous mind games! Let those who want COVID-19 medical treatment get that said treatment and leave the rest of us alone. Rational individuals who choose not to participate in a psychotic, demented, phobia-laced, COVID-19 clown world should not be subjected to the tyranny any longer.
***
Pg.61) “America has established a world-class surveillance operation, bolstering our ability to detect surges and emergence of new variants.”
Pg. 62) “America has also invested in global surveillance and built and strengthened international communication channels – including with United Nations organizations such as the WHO and networks of governments and scientists around the world – to understand and respond to COVID variants… The Administration stood up networks of government, and academic and company scientists to quickly conduct these assessments and provide real time information to policymakers and regulators… And during the last year, the Administration successfully built an emergency response infrastructure that the federal government can activate for future surges. Our surge response – led by FEMA and HHS – developed capabilities to stand up federal mass vaccination sites and federal testing sites; distribute critical supplies; and deploy thousands of federal clinical and non-clinical personnel to support states, Tribes, and territories to address critical needs on the ground, including addressing hospital personnel shortages, providing treatments, and administering vaccines. Since July 2021, the federal government has deployed over 4,000 military and non-military personnel to 46 states and territories… And if a new variant emerges, the federal government will leverage established playbooks to assess its impact on our vaccines, tests, treatments and deploy the tools, personnel and resources Americans need.”
The ambiguous choice of words, in this section, provides leeway for the government to implement dictatorial health measures for future COVID-19 outbreaks. Leaving words and phrases open to interpretation tells me that the current administration is actively pursuing their next power grab. What are the details behind these networks of government, academic, and company scientists who will be providing data to our policy makers and regulators? How do we know that said data is even accurate? What is the job description for federal non-clinical personnel? Specifically, what established playbooks does the administration plan to reference when a new variant emerges? We the people are not being afforded genuine government transparency as the administration talks down to us like we are children. How are we supposed to believe that the strategies and services discussed, within this section, are truly provided to us for our protection? As citizens, it is impossible to know if these measures are for our benefit due to lack of transparency. When governments blatantly dodge full disclosure, for scenarios that focus on the protection of its citizens, the only logical conclusion one can draw is that they are hiding something.
“Those, who would give up essential liberty to purchase a little temporary safety, deserve neither liberty nor safety.”—Benjamin Franklin
***
Thus far, we have covered 2/3rds of America’s National COVID-19 Preparedness Plan. Expect a riveting final part 3 briefing to be posted shortly.